Psychosis in Young Adults: Early Warning Signs
Recognizing the early signs of psychosis — especially in college students and young adults — can mean the difference between years of untreated illness and a life-changing intervention.
Psychosis is one of the most misunderstood conditions in mental health. Popular culture has shaped a distorted image — sudden, dramatic, unmistakable. The clinical reality is far more subtle. Most people who develop a psychotic disorder show warning signs months or even years before a full episode, and those early signs are frequently missed, dismissed, or misattributed to stress, substance use, or adolescent behavior.
For clinicians, families, and the young people themselves, understanding what early psychosis actually looks like is the first step toward earlier treatment, better outcomes, and reduced long-term disability.
The average duration of untreated psychosis (DUP) in the United States remains between one and two years. Research consistently shows that shorter DUP is associated with faster remission, lower relapse rates, and better functional recovery.
Who Is Most at Risk?
Psychotic disorders most commonly emerge in late adolescence and early adulthood — typically between the ages of 16 and 30. This window overlaps almost precisely with a major life transition: the college years. The combination of genetic vulnerability, neurobiological changes in the developing brain, social stress, disrupted sleep, and, often, increased substance exposure creates conditions in which psychosis can emerge in susceptible individuals.
Risk factors include:
A first-degree relative with a psychotic disorder (increases risk approximately tenfold)
A personal history of trauma or adverse childhood experiences
Cannabis use, particularly high-potency products, during adolescence
Social isolation or significant withdrawal from peers
A prior diagnosis of schizotypal personality disorder or prodromal symptoms
It is important to note that risk factors are not destiny. Many individuals with multiple risk factors never develop psychosis. The goal of identifying risk is not to pathologize normal development but to increase vigilance in those who would most benefit from early support.
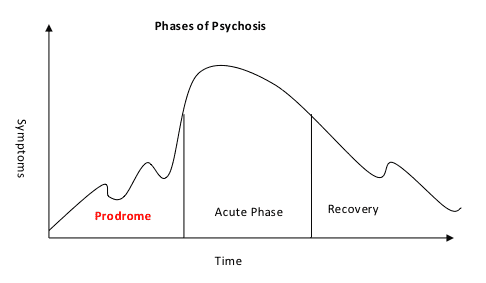
The Prodrome: What Comes Before Psychosis
The term prodrome refers to the period of emerging symptoms that precedes a first psychotic episode. During this phase — which can last weeks, months, or years — symptoms are often nonspecific and easy to rationalize.
Parents may notice their college student seems different: less motivated, more irritable, withdrawing from activities they once loved. Friends may observe that someone has become harder to read or oddly preoccupied. Academic performance frequently declines. The individual themselves may report that something feels off without being able to articulate what.
Clinically, the prodrome is characterized by attenuated (i.e., subclinical) versions of the psychotic symptoms that will later become overt. Recognizing these attenuated symptoms requires both clinical knowledge and a willingness to take them seriously.
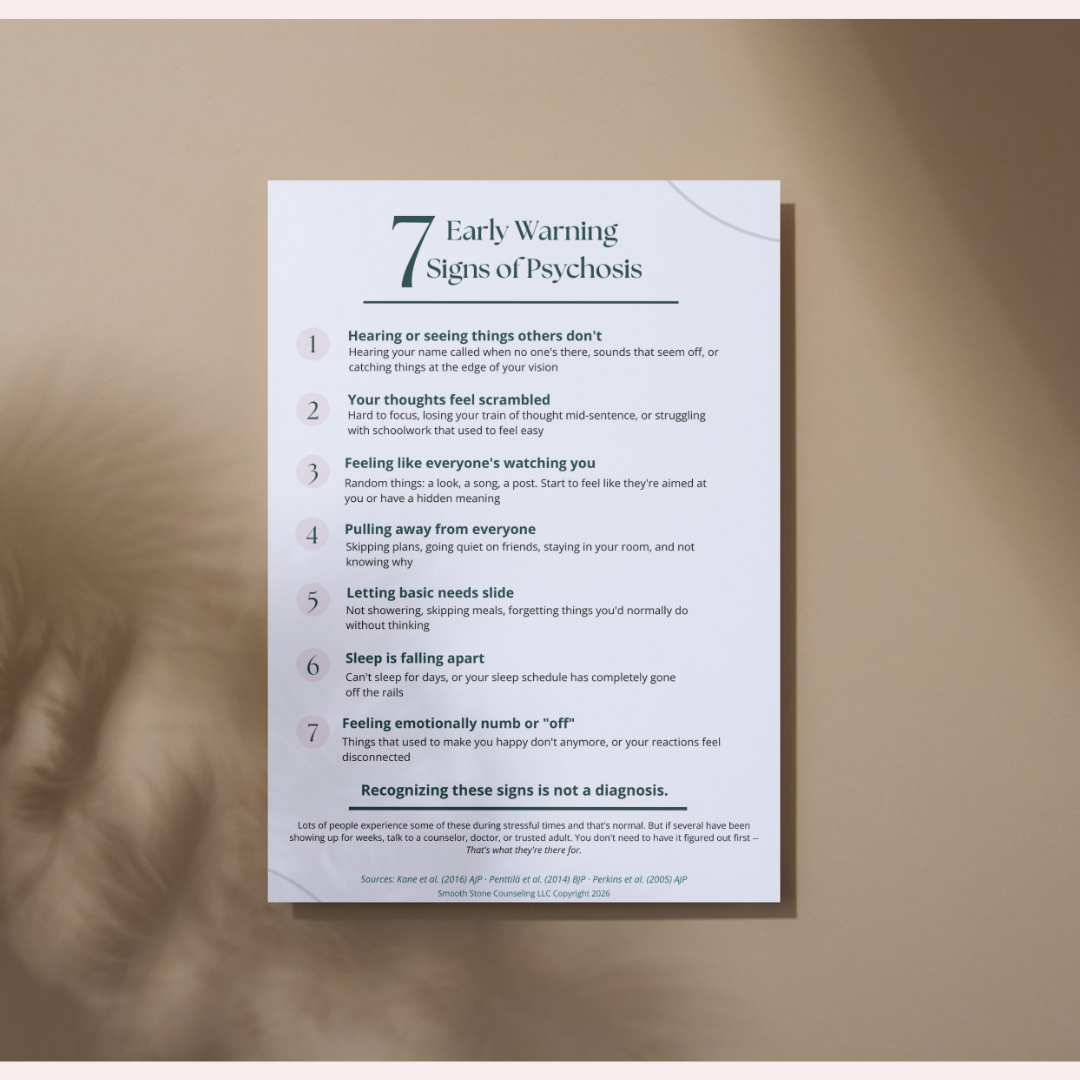
Early Signs of Psychosis to Know
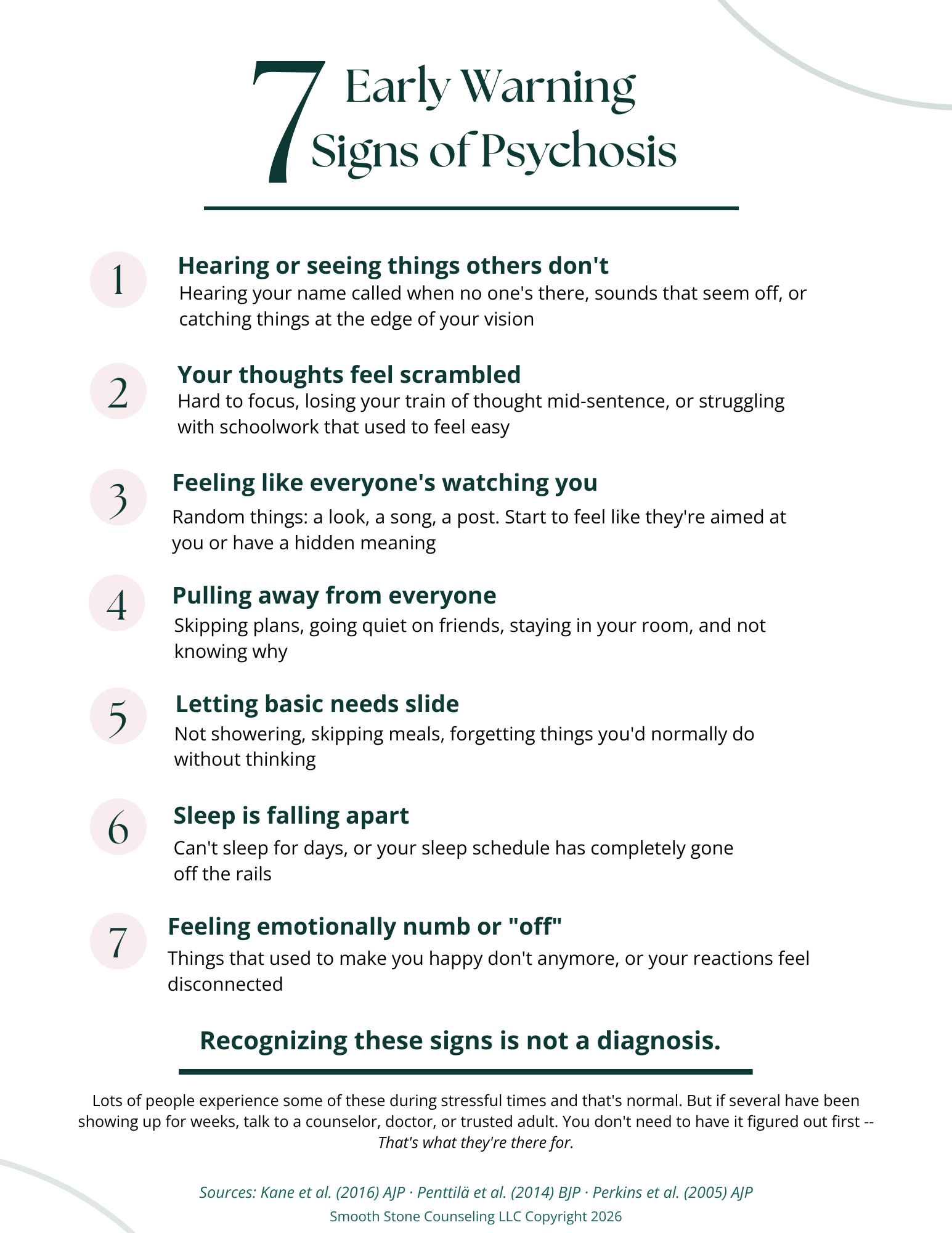
Download this hand out (click here)
1. Perceptual Disturbances
Early perceptual changes are among the most reliable prodromal signs, yet they are frequently underreported because individuals are often aware that their experiences are unusual and feel ashamed or frightened to disclose them.
Watch for:
Hearing sounds, voices, or one's name being called when no one is present — but with retained insight ("I know it's probably not real")
Heightened sensitivity to sensory input: lights seem too bright, sounds too sharp, textures unsettling
Fleeting visual disturbances: shadows at the periphery, objects appearing to shift or move
Tactile sensations without a clear physical cause
The retention of insight — knowing the perception is probably not real — is what distinguishes early prodromal experiences from frank hallucinations. This distinction matters for clinical assessment and should not be used to minimize what a young person is describing.
2. Disorganized or Unusual Thinking
Thought disorder is a hallmark of psychosis, but in its early form it is subtle. A college student's essays may become difficult to follow. Conversations may feel slightly off — as if the logical thread is looser than it should be. The person may struggle to complete complex tasks that were previously effortless.
Early cognitive signs include:
Difficulty concentrating or maintaining a train of thought
A sense that thoughts are "speeding up," slowing down, or becoming confused
Unusual or overly abstract ways of expressing ideas
Difficulty filtering irrelevant information from relevant information
Declining academic or occupational performance without an obvious external cause
3. Paranoid or Referential Ideation
One of the earliest and most clinically significant warning signs is the emerging sense that the world has become subtly threatening or meaningful in a personalized way. This is known as ideas of reference — the feeling that ordinary events (a passing car, a stranger's glance, a phrase on television) are somehow directed at or connected to oneself.
In early psychosis, this ideation typically has a tentative quality: the individual may say "I know it sounds strange, but it feels like people are watching me" or "I've been noticing a lot of coincidences lately that seem to mean something." The preserved doubt is clinically meaningful and should be directly explored rather than dismissed.
This is distinct from appropriate social anxiety or hypervigilance related to trauma — though those can coexist. A thorough assessment should explore the content, consistency, and conviction of these beliefs over time.
4. Significant Social Withdrawal
Social withdrawal is one of the most consistent and recognizable prodromal signs — and one of the easiest to attribute to other causes. A student who stops going to class, declines social invitations, and spends increasing time alone in their room may be depressed, overwhelmed, or exhausted. They may also be in the early stages of a psychotic disorder.
The nature and quality of the withdrawal matters. Early psychosis-related withdrawal often has an odd quality: the person may be preoccupied in a way that feels different from depression, may become vague or evasive about how they're spending their time, or may seem to be absorbed in an inner world that is difficult to access.
Social withdrawal paired with declining self-care, unusual preoccupations, or cognitive slippage warrants clinical attention — particularly in a young adult with known risk factors.
5. Decline in Self-Care and Functioning
A marked decline in hygiene, grooming, nutrition, or basic self-maintenance is a serious sign that something has changed. When a young adult who previously managed these things independently begins neglecting them consistently, and when this decline is accompanied by any other items on this list, it should be taken seriously.
This decline is not a character flaw or laziness — it reflects the real cognitive and motivational toll of emerging psychiatric illness. Negative symptoms such as avolition (diminished motivation) and alogia (reduced speech) can begin to emerge during the prodrome and represent early disruption of the systems that support goal-directed behavior.
6. Emotional Changes: Blunting or Inappropriateness
Affect — the observable expression of emotion — often changes in early psychosis. Families and friends may notice that the individual seems emotionally flat or muted: less animated, less expressive, laughing less. Others may notice the opposite: emotional responses that seem slightly mismatched to the situation.
These changes can be particularly confusing because they resemble depression and are often interpreted as such. The critical difference is that emotional blunting in psychosis tends not to be accompanied by the subjective suffering, hopelessness, or cognitive self-criticism characteristic of a depressive episode — though depression and psychosis certainly co-occur.
7. Sleep Disturbances
Sleep disruption both precedes and exacerbates psychotic symptoms. Severe insomnia — especially a complete inability to sleep for several days — is a recognized warning sign of an impending acute episode. More commonly, prodromal individuals experience a progressive shift in their sleep-wake cycle, hypersomnia, or fragmented sleep without a clear explanation.
Sleep and psychosis have a bidirectional relationship. Disrupted sleep can unmask or worsen psychotic symptoms, and emerging psychotic symptoms often disrupt sleep. Clinically, worsening sleep in the context of other prodromal signs should increase concern and urgency.
Psychosis in College Students: Why Campus Is a High-Stakes Setting
The college environment deserves specific attention. The late teens and early twenties represent peak onset risk for psychotic disorders, and universities concentrate large numbers of people in this exact demographic under conditions — stress, sleep disruption, substance exposure, social pressure — that can precipitate onset in vulnerable individuals.
Several features of campus life complicate early identification:
Behavioral changes may be attributed to adjustment difficulties, social anxiety, or homesickness
Academic decline may be assumed to reflect motivational or study skill problems
Substance use may mask or be seen as the primary cause of behavioral changes
The privacy of college living means parents may not observe changes until they are advanced
Stigma remains a significant barrier to help-seeking among young adults
Resident advisors, academic advisors, faculty, and campus mental health staff all represent potential points of early identification. Training these individuals to recognize prodromal signs — and to make warm referrals to clinical services — is one of the highest-yield prevention strategies available.
Campus counseling centers should be equipped to conduct structured prodromal assessments, such as the Structured Interview for Psychosis-Risk Syndromes (SIPS), and should have clear pathways to specialized early psychosis programs when indicated.
When to Seek Help and What to Expect
If you are a clinician, a family member, or a young person who recognizes several of the signs described above, the appropriate response is assessment — not a wait-and-see approach.
Early psychosis programs, increasingly available across the United States and internationally under the coordinated specialty care (CSC) model, offer evidence-based treatment tailored to young people in the early phases of illness. These programs typically include:
Psychiatric evaluation and, when indicated, low-dose antipsychotic medication
Individual therapy (particularly cognitive behavioral therapy for psychosis)
Supported education and employment services
Family education and support
Case management and care coordination
Research on coordinated specialty care programs — including the RAISE study conducted across the United States — has consistently demonstrated superior outcomes compared to treatment as usual, including faster symptom reduction, better medication adherence, and improved social and vocational functioning.
Early psychosis is not a life sentence. With timely, evidence-based treatment, many young people achieve remission and go on to pursue education, relationships, and careers consistent with their goals. The window for intervention matters enormously.
A Note on Language and Stigma
The language used to discuss psychosis matters. Terms like "crazy," "losing their mind," or "going off the deep end" reinforce stigma and make it less likely that young people will disclose their experiences or seek help. Clinicians, educators, and family members should model language that is clinical, accurate, and non-shaming.
Psychosis is a symptom — like fever or pain — that can arise from a range of conditions including schizophrenia spectrum disorders, bipolar disorder with psychotic features, major depression with psychotic features, and others. It is a medical phenomenon, not a moral failure, and it responds to treatment.
The goal of early identification is not surveillance or pathologizing normal variation. It is ensuring that young people who are struggling — who are frightened by experiences they don't understand, who are losing ground academically and socially — receive skilled, compassionate care before their illness becomes more entrenched.
If you are concerned about yourself or someone you know, contact a mental health professional, your campus counseling center, or the SAMHSA National Helpline at 1-800-662-4357. To locate an early psychosis program near you, visit the Early Psychosis Intervention Network (EPINET) at epinetwork.org.
This article is intended for educational purposes and does not constitute clinical advice. If you are experiencing a mental health emergency, call 988 (Suicide and Crisis Lifeline) or go to your nearest emergency department.
References:
Kane et al. (2016) — American Journal of Psychiatry — The flagship NIMH RAISE Early Treatment Program RCT; directly supports the CSC treatment section.
Penttilä et al. (2014) — British Journal of Psychiatry — A systematic review and meta-analysis on duration of untreated psychosis (DUP) as a predictor of long-term outcome; backs the DUP claim in the intro.
Perkins et al. (2005) — American Journal of Psychiatry — A widely cited meta-analysis on DUP and treatment response; provides the clinical evidence base for why early identification matters.
Arseneault et al. (2002) — BMJ — The landmark Dunedin cohort longitudinal study on adolescent cannabis use and adult psychosis risk; supports the cannabis risk factor point.
Di Forti et al. (2019) — Lancet Psychiatry — The large EU-GEI multicentre study on high-potency cannabis and first-episode psychosis incidence; adds a robust, recent citation for the cannabis-psychosis link.