Understanding Autism Spectrum Disorder: What Does “On the Spectrum” Really Mean?
A note before we begin: The field of autism research is evolving rapidly. This post reflects current understanding as of early 2025 and is intended as a general educational overview. Diagnostic criteria, terminology, and best practices continue to be refined. This blog is not a substitute for professional evaluation or individualized clinical advice.
What Is Autism Spectrum Disorder (ASD)?
Autism Spectrum Disorder (ASD) is a neurodevelopmental condition that affects how a person perceives, processes, and interacts with the world around them. The word “spectrum” is key — it reflects the wide range of ways autism can present across different people.
No two autistic people are the same. One person may be highly verbal and excel academically while struggling with social nuance. Another may be nonspeaking and require significant daily support. Both fall under the same diagnostic umbrella of ASD.
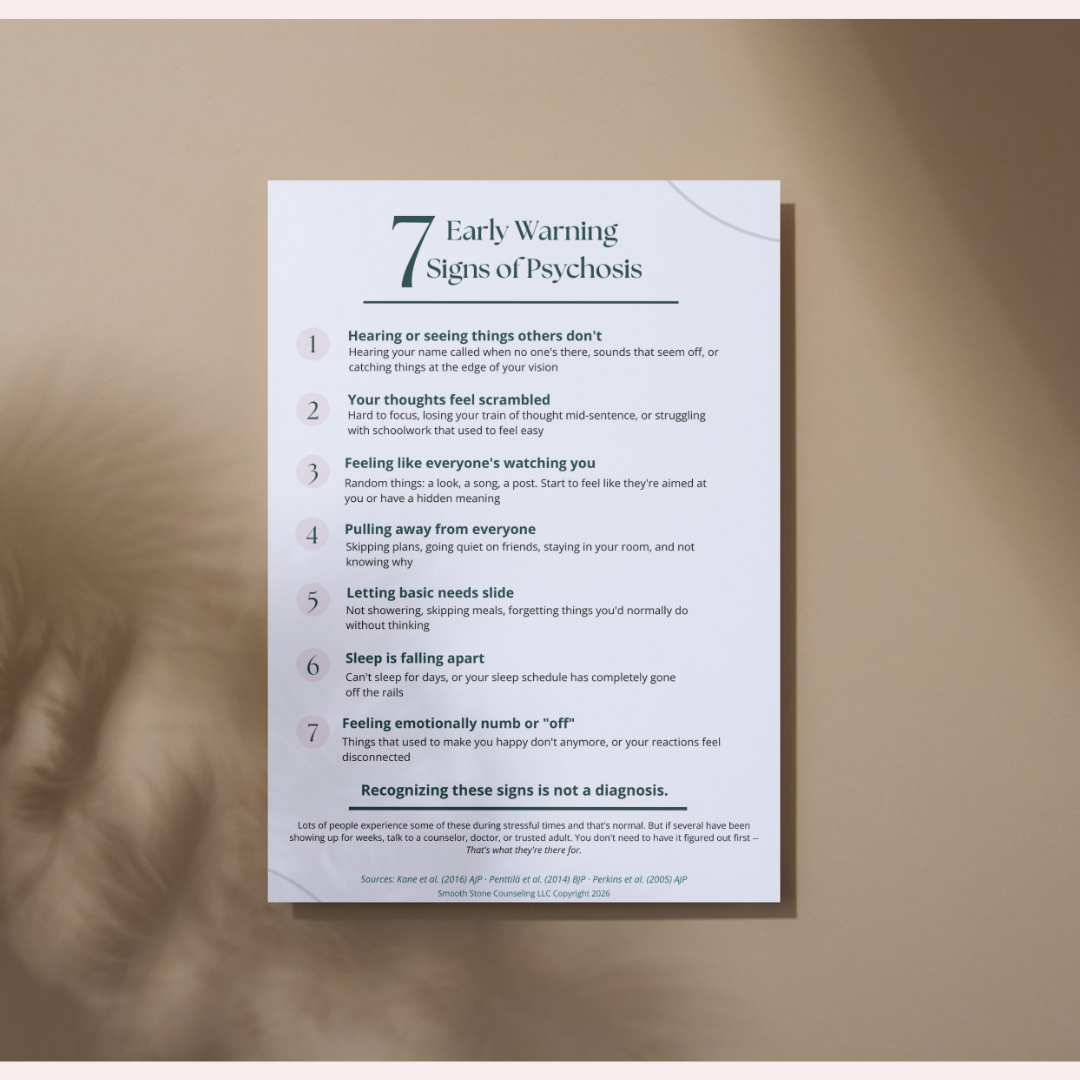
Autism is primarily characterized by differences in two core areas:
Social communication and interaction: including challenges with back-and-forth conversation, reading nonverbal cues, forming and maintaining relationships, and understanding social “unwritten rules.”
Restricted, repetitive behaviors and interests: including repetitive movements or speech, insistence on sameness, highly focused interests, and heightened or reduced sensitivity to sensory input.
These traits must be present from early development (even if not recognized until later in life) and must cause a meaningful impact on daily functioning to meet diagnostic criteria.
What Does “On the Spectrum” Mean?
In everyday conversation, people often say someone is “on the spectrum” as a shorthand for an ASD diagnosis. But what does that actually mean clinically?
Prior to 2013, several distinct diagnoses existed under separate labels, including:
Autistic Disorder
Asperger’s Syndrome
Pervasive Developmental Disorder – Not Otherwise Specified (PDD-NOS)
Childhood Disintegrative Disorder
With the publication of the DSM-5 (Diagnostic and Statistical Manual of Mental Disorders, 5th Edition), these were unified under the single diagnosis of Autism Spectrum Disorder. The intent was to better reflect the reality that autism is not a set of neatly separate conditions, but a continuum with significant variation.
⚠️ Important: Although the diagnostic labels have changed, many people who were diagnosed under the older system - particularly those with an Asperger’s diagnosis- still strongly identify with that terminology. This is valid and worth respecting in therapeutic settings.
The Spectrum Is Not a Line
One of the biggest misconceptions about autism is that the spectrum looks like a straight line from “mild” to “severe.” This is not accurate.
A more useful way to understand the spectrum is as a multidimensional profile. A person might have significant strengths in some areas (such as pattern recognition, memory, or focused expertise) and significant challenges in others (such as sensory regulation, executive function, or social interpretation). Their profile can also shift across different environments, stress levels, and life stages.
The spectrum means: the same core features, expressed in infinitely varied ways.
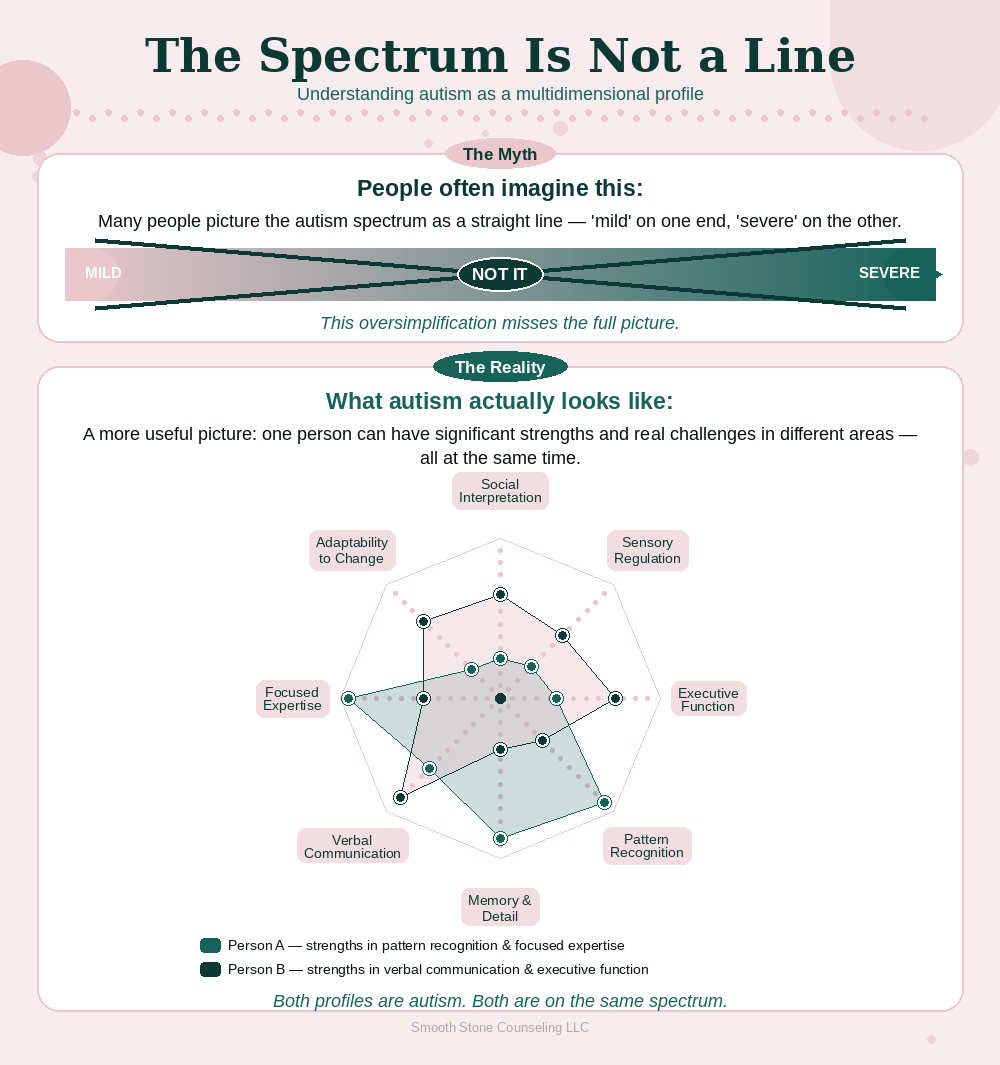
Image generated using Anthropic, Claude 2025
Levels of Support: The DSM-5 Framework
To communicate how much support an autistic person may need, the DSM-5 uses a three-level severity framework. These levels are based on the degree of support required - not on the person’s overall ability, intelligence, or worth.
Level 1: “Requiring Support”
Individuals at this level can often function with some independence but experience noticeable challenges that impact daily life without support structures. Common characteristics include:
Difficulty initiating social interactions or responding appropriately to others
Noticeable differences in communication that can make relationships challenging
Rigid thinking or routines that cause distress when disrupted
May be highly verbal but struggle with the “social” aspects of language (tone, subtext, humor)
Sensory sensitivities that may not be outwardly obvious
This level was previously most associated with what was called Asperger’s Syndrome or high-functioning autism, though both of those terms are now considered outdated in clinical use.
Level 2: “Requiring Substantial Support”
Individuals at this level experience more marked challenges in both social communication and behavior, requiring more consistent support. Common characteristics include:
Significant difficulty with verbal and nonverbal communication
Limited social initiation and reduced or atypical response to others
Inflexibility in behavior that is clearly noticeable and interferes with functioning
Difficulty coping with change, often resulting in distress
May have co-occurring language delays or differences
Level 3: “Requiring Very Substantial Support”
Individuals at this level require the most intensive support across settings. Common characteristics include:
Severe challenges in verbal and nonverbal communication; may be minimally verbal or nonspeaking
Very limited social interaction
Inflexibility of behavior causes extreme difficulty and distress
Significant difficulty with transitions and focus
May have co-occurring intellectual disability, though not always
A clinical note: Support levels can change over time and across contexts. A person assessed at Level 2 in childhood may develop coping strategies and supports that shift their daily functioning significantly. Levels describe current support needs, not fixed traits or potential.
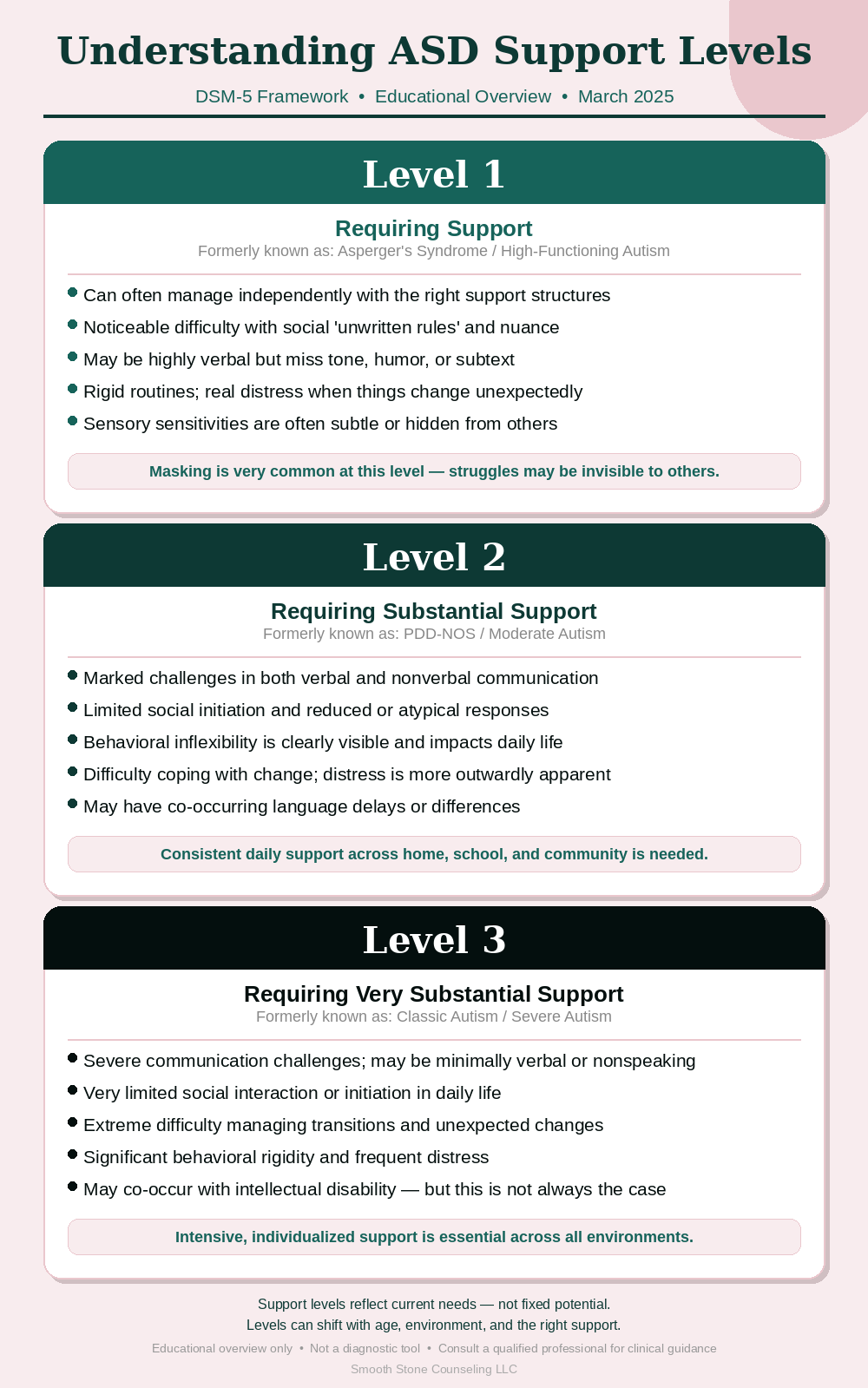
Image generated using Anthropic, Claude 2025
Common Co-Occurring Conditions
ASD rarely appears in isolation. A wide range of co-occurring conditions are common and can significantly shape a person’s experience. Recognizing these is essential to accurate diagnosis and effective support.
ADHD — extremely common alongside ASD; affects attention, impulse control, and executive function
Anxiety disorders — generalized anxiety, social anxiety, and OCD are frequently seen
Depression — particularly in adolescents and adults who have struggled without diagnosis or support
Sensory Processing Differences — hyper- or hyposensitivity to sound, light, texture, taste, or touch
Sleep difficulties — reported in a significant portion of autistic individuals
Intellectual disability — present in a subset of autistic people; not a universal feature of ASD
Gastrointestinal issues — emerging research suggests higher prevalence in autistic populations
Epilepsy / seizure disorders — co-occurs at higher rates than in the general population
Language and communication disorders — including apraxia of speech
Understanding the full diagnostic picture is critical; treating anxiety or ADHD in isolation, without recognizing the underlying autism, often leads to incomplete or ineffective care.
How Is ASD Officially Diagnosed?
There is no blood test, brain scan, or single definitive medical test for autism. Diagnosis is clinical - meaning it is based on observation, history, and standardized assessment by a qualified professional.
Who Can Diagnose ASD?
A formal ASD diagnosis in the United States can be given by:
Psychologists (clinical, developmental, neuropsychologists)
Psychiatrists
Developmental pediatricians
Neurologists with developmental training
Some licensed clinical social workers or other clinicians, depending on state licensing and scope of practice
The most thorough evaluations are typically conducted by neuropsychologists or developmental specialists, and often involve a team-based approach.
What Does the Evaluation Process Look Like?
A comprehensive autism evaluation typically includes:
Developmental history interview with the individual and/or family
Structured observation of behavior (such as the ADOS-2 — Autism Diagnostic Observation Schedule)
Parent/caregiver interview tools (such as the ADI-R — Autism Diagnostic Interview-Revised)
Cognitive and intellectual testing
Language and communication assessment
Adaptive behavior assessment (how the person functions in daily life)
Screening for co-occurring conditions
Evaluations in adulthood can look different from those in childhood, as many adults — especially women, girls, and people of color — have developed strong masking* strategies that can obscure autistic traits during observation.
*On masking: Many autistic individuals, particularly those not diagnosed in childhood, have learned to “mask” or camouflage their autistic traits to fit in socially. This can make adult diagnosis complex and can result in significant mental health costs for the individual. A skilled evaluator takes masking into account.
The Benefits and Complications of an Official Diagnosis
The question of whether to pursue a formal ASD diagnosis is deeply personal. There are real advantages and real tradeoffs worth understanding before making the decision.
Potential Benefits of an Official Diagnosis
Self-understanding: A diagnosis can offer profound relief, validation, and a new framework for understanding a lifetime of experiences.
Access to services: In school settings, an ASD diagnosis can open the door to IEPs (Individualized Education Programs), accommodations, and specialized support.
Workplace accommodations: Under the Americans with Disabilities Act (ADA), a diagnosis may support requests for reasonable workplace accommodations.
Access to therapies: Many insurance plans and state-funded programs require a formal diagnosis to cover services such as Applied Behavior Analysis (ABA), speech therapy, occupational therapy, and social skills groups.
Community and identity: Many autistic individuals find deep connection and belonging in the autistic community, which is often accessed after a diagnosis.
Legal and Systemic Implications to Know
A formal ASD diagnosis is a medical record, and like all medical records, it has both protective and potentially complicating dimensions. It’s important to be informed.
Protective Legal Applications
Disability protections under the ADA and Section 504 of the Rehabilitation Act apply to autistic individuals in educational and workplace settings.
The Individuals with Disabilities Education Act (IDEA) entitles eligible children to a free and appropriate public education, including specialized services.
SSI/SSDI disability benefits may be accessible to autistic individuals who meet functional criteria.
Certain legal matters — such as guardianship proceedings, custody evaluations, or criminal defense contexts — may be influenced by a documented diagnosis.
Areas Where Diagnosis May Introduce Complications
Insurance: A formal diagnosis becomes part of your medical record. While the ACA prohibits denial of coverage for pre-existing conditions, this landscape can shift, and some life insurance or disability policies may be affected.
Employment: While the ADA offers protections, stigma around mental health and neurodevelopmental diagnoses can unfortunately, influence hiring in informal ways. Disclosure is always the individual’s choice.
Military service: An ASD diagnosis may disqualify individuals from certain branches or roles in the military.
Immigration: Disability-related diagnoses can, in some circumstances, be considered during immigration proceedings, particularly if they are associated with a documented need for significant public support.
Parental rights and custody: In family law proceedings, a diagnosis can be used constructively or, in some unfortunate cases, weaponized. The context and framing matter greatly.
Legal note: This blog is for general informational purposes and is not legal advice. If you are navigating situations involving law, disability rights, custody, or benefits, consulting with a disability rights attorney is strongly recommended. Laws vary by state and are subject to change.
What If You Don’t Want a Formal Diagnosis?
Some people explore the idea of autism and come to a place of self-identification or “community diagnosis,” recognizing themselves in the autism experience without pursuing formal evaluation. This is a valid personal choice and is widely accepted within the autistic community.
That said, self-identification does not carry legal weight and will not qualify a person for disability accommodations, services, or benefits. Therapists and other providers can still offer supportive, autism-affirming care to self-identified individuals, while being transparent about what a formal evaluation can and cannot provide.
A Note on Language and Identity
Language around autism is evolving and can be a meaningful topic for autistic individuals and families. There are two main camps:
Identity-first language (“autistic person”) — preferred by many in the autistic community, reflecting the view that autism is an integral part of who they are.
Person-first language (“person with autism”) — preferred by some individuals and families who wish to separate the person from the diagnosis.
There is no universally correct answer. The respectful approach is to follow the preference of the individual or family.
Final Thoughts
Autism Spectrum Disorder is not a puzzle to be solved — it is a different way of being in the world. For many autistic individuals, the greatest challenges are not autism itself, but a world not designed with them in mind, and the lack of understanding, support, and acceptance they have encountered along the way.
Whether you’re a parent seeking answers, an adult exploring your own neurology, or a person supporting someone on the spectrum, understanding what ASD really is — beyond the stereotypes and shorthand — is one of the most valuable things you can do.
Smooth Stone Counseling is committed to neurodiversity-affirming care.
This post will be updated as diagnostic criteria, research, and best practices evolve. Please contact us for concerns and updates. Last reviewed: March 2025.